You are here
A Hidden Solution for Clearer Hearing

Indication: Mild to severe sensorineural deafness, or mixed deafness with a moderate to severe sensorineural deafness component.
Mild to severe sensorineural deafness is effectively amplified by a Vibrant Soundbridge Middle Ear Implant, with better responses especially in the high frequencies compared to a conventional hearing aid.
One of the other advantages of the MIddle Ear Implant is that it bypasses the ear canal and the problems that can occur from using a hearing aid. A hearing aid blocks the ear canal to varying extents creating an occlusion effect, or the opposite if not tight enough results in whistling feedback. It can also create discharge problems if there is otitis externa (swimmers ear) or a mastoid cavity, and cannot be used if there is ear canal atresia (abscence) / severe stenosis (narrowing).
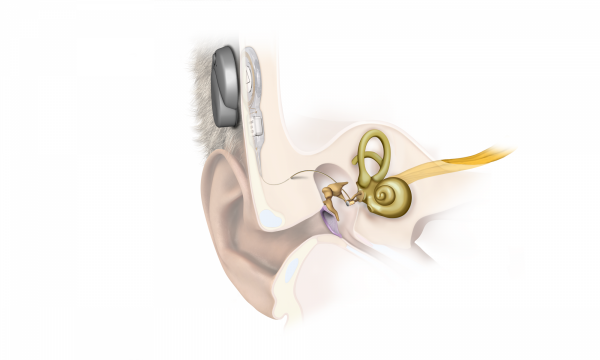
Surgical steps are similar to a Cochlear Implant. However there is no surgery to the inner ear (cochlea) and instead of this, a vibrating Middle Ear Implant is implanted into the middle ear, attached to one of the Ossicles, Round Window or Oval Window.
The Vibrant Soundbridge device is implanted under the skin, with an external combined microphone and processor (a slim circular discreet device) held by magnetic interface to the internally implanted component hidden above the hair line.
Left Vibrant Soundbridge (VSB) Middle Ear Implant with KTP Laser-Assisted Middle Ear Reconstruction surgery performed by Dr Arasa Raj Sinnathuray
PRE-OP
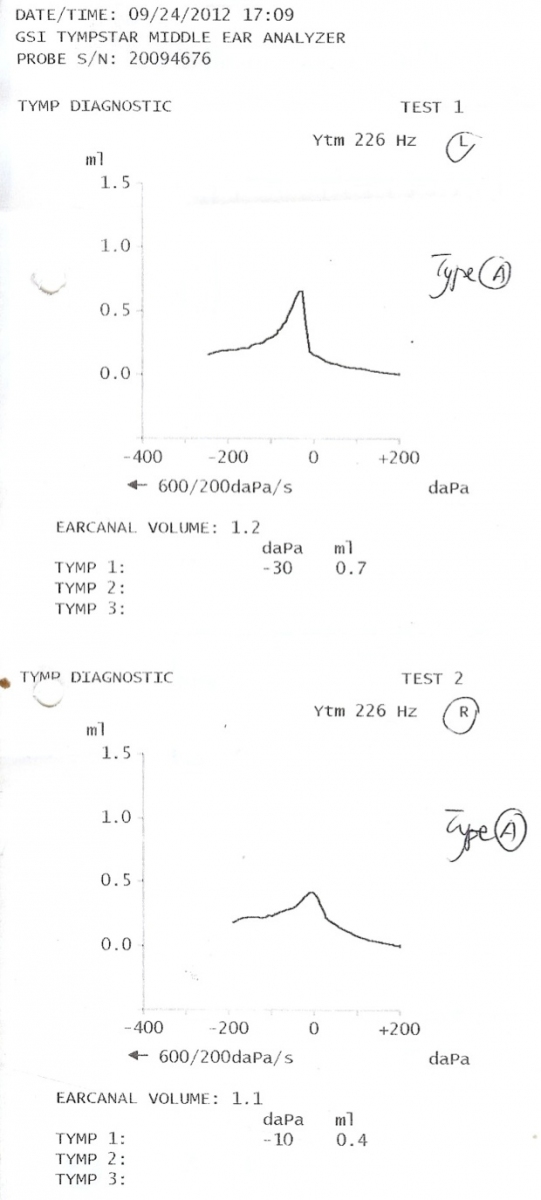
This patient was a 22-year old male with a traumatic bomb blast injury to his left ear drum and left > right deafness, left-only non-pulsatile tinnitus, discharging ears, and right ear pain. Examination revealed on the right a retracted and scarred pars tensa (mid- and lower ear drum) and clean attic pocket (upper ear drum). On the left (pictures shown below) there was a thin retracted membrane replacing nearly the entire pars tensa (mid- and lower ear drum), and a dislocated Incus (also known as the Anvil middle ear bone) situated anterior to the Malleus (also known as the Hammer middle ear bone), ie in the wrong position. Tympanograms (middle ear and ear drum integrity test) were normal but an Audiogram (hearing test) revealed a left mixed (conductive and sensorineural) mild hearing loss across the speech frequencies, with bilateral high frequency sensorineural deafness. He was initially treated with conservative treatment including keeping the ears dry, antibiotic-steroid ear drops and a left open-fit hearing aid. The left hearing aid helped with his hearing and tinnitus, but the left ear continued to discharge.
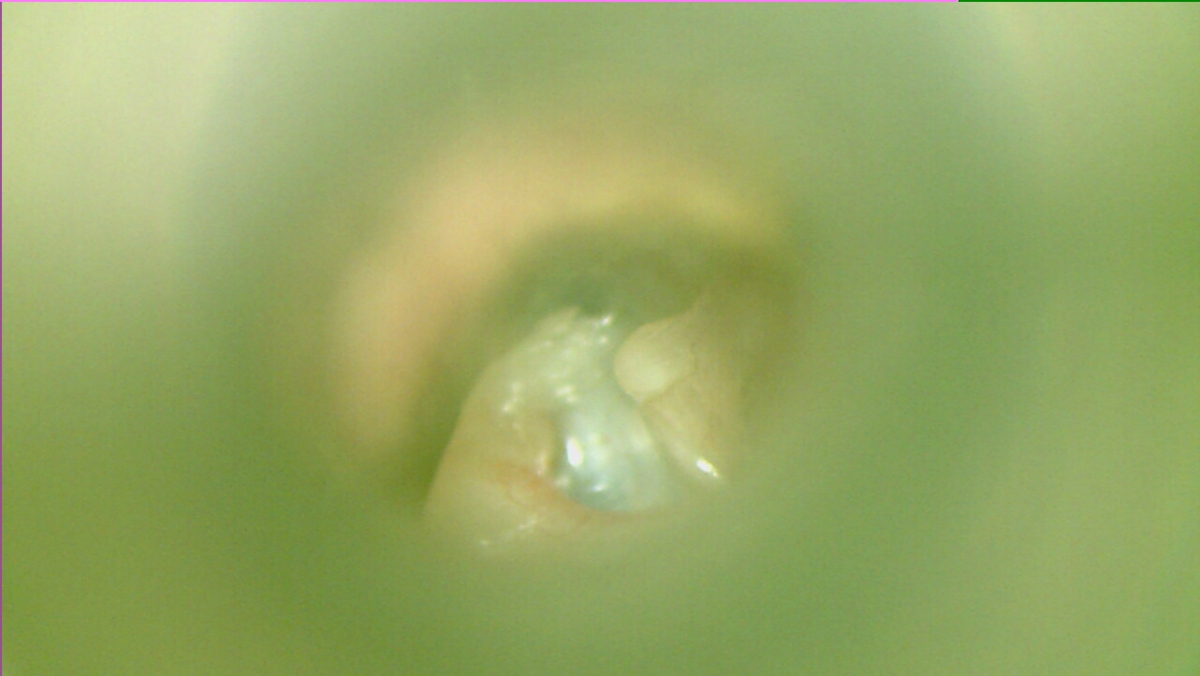 Pre-op Left upper Ear Drum showing Dislocated Incus (Anvil)
Pre-op Left upper Ear Drum showing Dislocated Incus (Anvil)
 Pre-op Left mid-Ear Drum
Pre-op Left mid-Ear Drum
 Pre-op Left lower Ear Drum
Pre-op Left lower Ear Drum
AUDIOLOGY: Pre-op Tympanogram
The perisitent left ear discharge was felt to be secondary to his severely retracted left ear drum and hearing aid-worsened otitis externa (ear canal inflammation). To overcome the ear drum problem, a cartilage tympanoplasty (ear drum reconstruction) was proposed, but due to the resultant increased conductive loss together with the need for amplification without ear canal irritation, a Vibrant Soundbridge (VSB) Middle Ear Implant was simultaneously proposed. He underwent a preoperative CT scan which detected no abnormality other than the dislocated Incus (Anvil). However in the Operating Theatre he was also found to have implantation Cholesteatoma (chronic invasive middle ear disease), with extensive middle ear scarring and granulation tissue on the Stapes footplate (also known as the Stirrup middle ear bone), as well as no Stapes suprastructure (Stirrup arch). Pre-operative middle ear sound conduction was probably assisted via this disease tissue. After Cholesteatoma removal, a KTP laser was used to gently vaporise the scarring and granulations, to reduce the risk of secondary inner ear trauma from dissection of this disease. The ear drum was posteriorly reconstructed with cartilage and the VSB device was applied directly to the Stapes (Stirrup) footplate, stabilised with a Vibroplasty Coupler.
PROCEDURE: Left KTP-Laser Asssited Combined Approach Tympanoplasty + Vibrant Soundbridge Middle Ear Implant with Clip Coupler
POST-OP
A couple of months after surgery the left ear canal and drum had healed well (picture shown below). The VSB underwent programming. A postoperative unactivated Implant Audiogram revealed the Bone Conduction (Inner ear) levels to have improved compared to preoperatively (probably secondary to a Cahart effect). An early Implant-aided Audiogram revealed a threshold of 31.25 dB comparable to the preoperative Air Conduction level, and this improved further over time. The patient was happy with the hearing and felt it to be symmetrical / balanced. There was no more ear discharge and he could let water into the ear, including swimming.
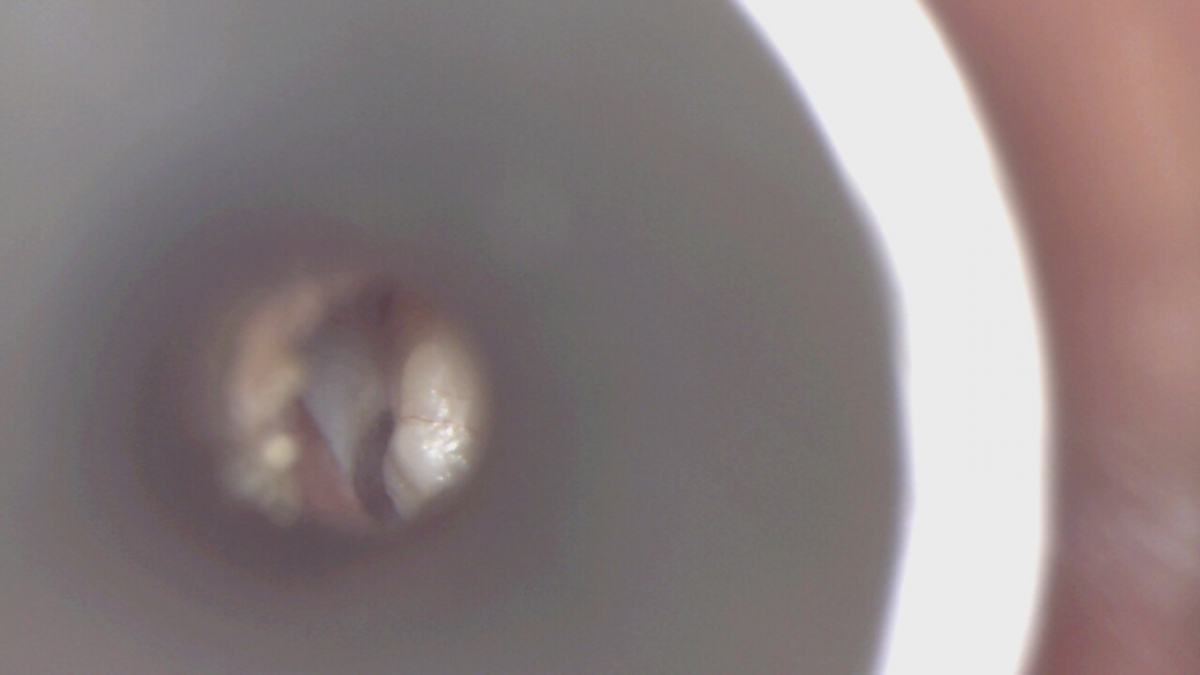 Post-op Left Ear Drum with Cartilage Reconstruction
Post-op Left Ear Drum with Cartilage Reconstruction
AUDIOLOGY: Post-op Unactivated Implant Audiogram
(Early) Post-op Implant Activated Left Audiogram
See Media: https://otologypro.com.my/media

{kind=link}